Mental Health Recovery Mission Training Report - Independent Evaluation Report 2023
 Wellbeing
Wellbeing  Suicide prevention
Suicide prevention 
Report
Updated: 29/09/2023
PDF download
Download a designed version of this report in PDF.
Executive Summary
There is a growing body of evidence that health inequalities are now widening and that the cost-of-living crisis, poverty and financial stress will likely rise over the next few years. The Mental Health Foundation report (1) states that the effects of the cost-of-living crisis on public mental health will be on a scale similar to the COVID-19 pandemic and that concerns about finances are having a negative effect on people’s ability to engage in some of the activities known to help protect mental health.
As part of the Mental Health Recovery Mission, one of the Mayor of London’s nine missions developed for London’s recovery from the pandemic, Thrive LDN worked with their ‘Economic Wellbeing Forum’ (2) to identify and co-create a range of mental health training offers to support Londoners during winter 2022/23 and beyond. The aim of the training offers was to build and strengthen resilience by diversifying and scaling mental health training offers in London. A budget of up to £90,000 (inc. VAT) was made available to deliver three bespoke training programmes: Trauma Informed Practice, Mental Health Awareness and Core Conversations (training to support people to help others). This evaluation was designed to explore the reach and impact on training participants.
Programme reach
The training was accessed by people such as frontline workers and those in a position to support others, building capacity to increase support for mental health and wellbeing. In total, at the time of the evaluation, 2,790 participants registered on one or more of the training programmes. Of these 2,168 attended the training. The majority (83%) of participants were female, working in the public and voluntary sectors with high representation from ethnically diverse populations. Whilst all London boroughs had participants attend the training offer (an average of 50 per borough), there were significant differences in the numbers of participants by borough. Some boroughs with high levels of need were underrepresented.
Programme impact
Through pre and post participant surveys, we looked to understand the impact of the training on participants knowledge, confidence and attitudes. The evaluation found that the majority of participants already had extensive experience and knowledge in the subject matter, however these increased further post training, as reflected in the tables below.

Participants overall rating of training effectiveness
The reported effectiveness of all three training programmes in meeting the participants’ needs was very high. Over seven-in-ten participants of the Mental Health Awareness and Core Conversations training and nine-in-ten of the Trauma Informed Practice participants rating it ‘very’ or ‘totally’ effective. Additionally, the evaluation found a strong willingness of participants to use the training in their practice.
Summary
The evaluation was able to evidence that there was clear synergy between programmes, making them feel like it was a coherent package of training. There was a very clear demand for the training programmes and to meet this demand it is encouraging that sustainability of the training offer was considered and built in from the outset, with much of the training resource provision still accessible to a wider audience online.
The evaluation has evidenced significant short-term impacts of the training on participants knowledge and confidence and their intent to put the training into practice. There was also a clear demonstration of participants using the training to cascade to a wider audience within their local area or within their own organisation. The limitations of the evaluation meant it was not able to quantify this reach.
Recommendations
Some fine tuning to the training offers, going forward, could help to ensure that its reach and positive impact in practice is even more widespread in the future. The report provides six broad recommendations (in no particular order) for the commissioners to consider.
Recommendation 1: Continue to provide a training offer in this field
Recommendation 2: Further develop the marketing and promotion of the training
Recommendation 3: Minimising programme drop off
Recommendation 4: Broadening the training offer
Recommendation 5: Develop the evaluation methodology to gather longer term outcomes
Recommendation 6: Share the learning
–
(1) https://www.mentalhealth.org.uk/explore-mental-health/statistics/people-physical-health-conditions-statistics#:~:text=More%20than%2015%20million%20people,also%20have%20mental%20health%20problems.
(2) The Economic Wellbeing Forum is an online forum with membership from across statutory health and social care partners and voluntary and community sector organisations. The Forum was set up with the specific intention of focusing efforts and offers of support on those from the lowest socio-economic backgrounds and/or belonging to communities which have historically been marginalised and socially excluded.
1. Introduction to the Report
The London Recovery Board (a partnership of leaders from across London’s government, business, civil society, and other key sectors) was tasked with coordinating the planning for London’s future post-COVID. The London Recovery Board takes a Missions Based Approach and has defined nine missions for London’s recovery from the pandemic, one of which is the Mental Health Recovery Mission (MHRM) (3). The mission includes improving Londoners access to resources that will equip them with the tools they need to support those around them, ensuring that there is an emphasis on resilience-building programmes and preventative programmes for disproportionately impacted groups.
1.1 The Mental Health Recovery Mission Training
As part of the Mental Health Recovery Mission, Thrive LDN worked with their ‘Economic Wellbeing Forum’ (4) to identify and co-create a range of mental health training offers to support Londoners during winter 2022/23 and beyond. The aim of the training offers was to build and strengthen resilience by diversifying and scaling mental health training offers in London.
A £90,000 (inc. VAT) budget was made available to deliver three bespoke training programmes. Specifications were drawn up and sent out to tender, resulting in three private training providers being selected to deliver the following:
- Trauma Informed Practice (Nicola Lester Ltd). Training focused on supporting participants working across a range of contexts to develop trauma informed approaches within their role. The training was accredited, and participants had the opportunity to receive a certificate on completion of each module. The modules included: (1) Becoming Trauma Aware (Bronze Level) (2) Developing Trauma Informed Practice (Silver Level) and Committed to Trauma Informed Practice (Gold Level). The objectives were for participants to: gain an understanding of trauma and its impact on a person and their state of being
- appreciate the key principles of trauma-informed practice and how to apply them in real-life settings across a range of contexts
- gain an understanding of how to structure trauma-informed interventions, programmes, and organisations
- learn how to protect against vicarious trauma and promote self-care for professionals and their organisation.
- Mental Health Awareness (Healthy Dialogues Ltd). Training for frontline workers who are in direct contact with people that need support for cost-of-living pressures. The training was delivered online in three modular sessions (A) What is mental health and where to find support (B) Having conversations about mental health (C) How to support someone experiencing a mental health crisis. The objectives were for those working on the frontline to: gain an understanding of the psychosocial model of mental health and wellbeing
-
- improve their mental health literacy and knowledge including stigma related to financial hardship
- recognise where and when to get further information and support
- understand what to do in an urgent situation when someone is experiencing an emotional or mental health crisis.
- Training to support people to help others. Core Conversations (Basis Ltd): Training designed to enable people to feel more confident in the technique and practice of having conversations regarding mental health and well-being offering five pan-London sessions and 15 Local Authority sessions. All participants in the Local Authority sessions were offered the opportunity to take part in train-the-trainer sessions. This enabled an upskilling offer to be included in the programme and providing a sustainable offer for the Local Authority to continue to reach more Londoners after the training contract had ended. The objectives of the Core Conversations training were to support Londoners to feel confident to engage in conversations with friends, family or those in their community or workplace about mental health and wellbeing through developing: active listening and conversation skills
- an understanding how to start, maintain and close a conversation around mental health
- an ability to use gentle questioning and suggestions on mental health and wellbeing
- an understanding of how to encourage help-seeking behaviour and tackle stigmatisation of financial wellbeing
- knowledge of mental health resources and where to signpost for support
All three training programmes were delivered online, rather than face to face, with Core Conversations and Mental Health Awareness delivered as ‘live’ sessions and Trauma Informed as a pre-recorded video format, with the inclusion of a British Sign Language interpreter. It was anticipated that offering pre-recorded video modules would enable a wider range of participants to take part in the training post contract, leading to sustainability going forwards.
-
-
- if and how the training offers worked in practice
- the effectiveness of each training programmes performance and impact
- their value to participants and stakeholders
-
1.2 The Evaluation Report
In January 2023, through funding by the Mayor of London, Thrive LDN commissioned ‘Progress Health Partnerships Ltd’ to conduct an independent evaluation of the training offer. The evaluation was designed to help Thrive LDN and their partners understand:
- if and how the training offers worked in practice
- the effectiveness of each training programmes performance and impact
- their value to participants and stakeholders
-
This report briefly outlines the context of mental ill health across London, it highlights the theory of change underlying the programme and presents the output and outcome data gathered from the training participants. The report draws on the findings to help identify key lessons learned and makes recommendations for future training provision.
_
(3) https://www.london.gov.uk/sites/default/files/recovery_programme_overview.pdf
4 The Economic Wellbeing Forum is an online forum with membership from across statutory health and social care partners and voluntary and community sector organisations. The Forum was set up with the specific intention of focusing efforts and offers of support on those from the lowest socio-economic backgrounds and/or belonging to communities which have historically been marginalised and socially excluded.
2. The Context Behind The Training
The UK is currently in the grips of a well-documented cost-of-living crisis, which has seen the highest rate of inflation in 40 years and the largest drop in household disposable income in over a century. This has followed hot on the heels of the COVID-19 pandemic and together we know that this has significantly increased the number of people with ‘lived experience’ of financial worries and mental health issues. This includes Londoners with depleted financial resilience, and no capacity to save and prepare for future economic shocks, placing them at an increased risk for anxiety, cumulative stress and mental health issues.
2.1 The size of the problem
An estimated 4 million people in England suffer from poor mental health (5) and over half a million people in England are currently living with severe mental illness, such as psychosis or bipolar disorder (6). Studies in the UK and elsewhere indicate that people living with these severe mental health problems may die up to 20 years earlier than the general population (7). Poor mental health is also closely associated with many forms of inequalities, including poverty, unemployment, homelessness, incarceration, and social isolation.
Amongst older adults (55+ yrs), on average, depression affects 22% of men and 28% of women, yet an estimated 85% of older people with depression receive no help from the NHS (8). Of people aged 65 and over, over half a million (579,803) experience anxiety disorder, with a larger proportion of these challenges experienced by women more than men (9). Major life events such as bereavement, loneliness, retirement, and comorbidities have the potential to influence the mental health and wellbeing of older Londoners (10). According to Age UK, many older people find it difficult to discuss their mental health and this influences whether they reach out for support or not after a major life event (11).
The Mental Health Foundation have recently reported that the UK population is experiencing widespread levels of stress, anxiety and hopelessness in response to financial concerns. In a survey of 3000 adults conducted at the end of 2022, they found that 29% of adults experienced stress, 34% experienced anxiety and 10% said they felt hopeless because of financial worries during the previous month (12).
Londoners have the worst mental health out of all the regions of the country. Two million Londoners experience some form of poor mental health every year and Londoners’ life satisfaction and feelings of self-worth are lower than the national average (13). In 2014, the only year in which reliable data is available, an estimated 1 in 6 adults in London had experienced a common mental health disorder (CMD) such as depression and anxiety. This prevalence rose by one fifth between 1993 and 2014 (when the last survey was completed) and it is thought that the impact of Covid-19 and the current cost of living crisis will have significantly increased these numbers. The latest estimates from the Public Mental Health Dashboard placed the estimated rate of common mental disorders, at just below 20% of all Londoners (14).
The impact of structural racism and discrimination on mental health and wellbeing is clear. People identifying as ‘Black and Black British’ were more likely than average to have experienced CMD (23%) with ‘White British’
and ‘White Other’ people less likely (17% and 14% respectively). They were also disproportionately affected by the COVID-19 pandemic. The COVID-19 Social Study (15) found that people from ethnically diverse backgrounds consistently showed higher levels of anxiety and depression throughout the pandemic in comparison to their white counterparts. These outcomes are inextricably linked to the wider determinants of health, as those from ethnically diverse and minority communities are more likely to suffer from lower financial resilience and poverty, less likely to have access to green spaces and are more likely to live in densely populated or overcrowded housing (16).
Economically inactive and unemployed people were substantially more likely to have experienced a CMD in the last week (33%) than those who are in work (14%). A survey of chairs and chief executives of mental health trusts found that 98% of responders believe financial hardships add pressures to mental health services (17). Alongside this, social isolation and loneliness are major factors affecting mental health and this is a particular issue in the capital. The recent comprehensive Survey of Londoners (18) showed that, on average, eight per cent of Londoners feel lonely always or often.
There is variation in the rates of common mental health disorders across the London boroughs, with inner east London boroughs having the highest prevalence and most outer London boroughs having the lowest. A total of 23 out of London’s 33 boroughs are above the national average for CMDs. The lowest level of mental health prevalence is 13.2% in Richmond and the highest is 24.4% in Hackney and 23.9% in Newham.
Table 1: London boroughs with highest and lowest prevalence of CMD (19)

–
5 https://www.mentalhealth.org.uk/explore-mental-health/statistics/people-physical-health-conditions-statistics#:~:text=More%20than%2015%20million%20people,also%20have%20mental%20health%20problems.
6 https://ukhsa.blog.gov.uk/2018/12/18/health-matters-reducing-health-inequalities-in-mental-illness/
7 https://www.gov.uk/government/publications/health-matters-reducing-health-inequalities-in-mental-illness/health-matters-reducing-health-inequalities-in-mental-illness
8 https://www.mentalhealth.org.uk/explore-mental-health/statistics/older-people-statistics
9 https://www.ageuk.org.uk/latest-press/articles/2022/large-numbers-of-older-people-could-do-with-some-mental-health-support—but-are-less-likely-than-younger-groups-to-receive-it/
10 Thrive LDN. Intersectional Equity: Navigating protected characteristics. Evidence Briefing
11 https://www.ageuk.org.uk/latest-press/articles/2022/large-numbers-of-older-people-could-do-with-some-mental-health-support—but-are-less-likely-than-younger-groups-to-receive-it/
12 https://www.mentalhealth.org.uk/about-us/news/stress-anxiety-and-hopelessness-over-personal-finances-widespread-across-uk-new-mental-health-survey
13 https://www.london.gov.uk/sites/default/files/gla_migrate_files_destination/Mental%20health%20report.pdf
14 https://thriveldn.co.uk/evidence-and-insights/evidence/indicators-of-population-mental-health/#_ftn1
15 University College London (2021) Covid-19 Social Study: https://www.covidsocialstudy.org/results
16 Thrive LDN. Intersectional Equity: Navigating protected characteristics. Evidence Briefing
17 https://healthcareleadernews.com/news/financial-hardship-and-loneliness-drive-up-mental-health-demand-nhs-leaders-warn/
18 https://www.london.gov.uk/programmes-strategies/research-and-analysis/people-and-communities/survey-londoners
19 https://www.mylondon.news/news/zone-1-news/london-boroughs-youre-most-likely-17598684
3. The Evaluation Methodology
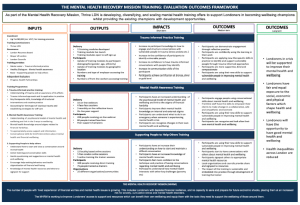
The evaluation has been designed to help inform delivery of future training offers and explores the programmes reach into the targeted populations and its impact on participants. The evaluators (Progress Health Partnerships) were brought in from the outset and have worked with Thrive LDN and the training providers to co-design an outcomes framework for the training (Fig 1).
The evaluation methods focused on gathering new quantitative and qualitative data over an eight-month period and included secondary analysis of existing quantitative data gathered by the training provider. The methodology was split into a series of inter-connected work-packages as follows:
- Understanding the context behind the training programme: Desk based research to investigate the current and planned delivery models and agree key stakeholders for the evaluation.
- Development of an outcomes framework: Development of a robust outcomes framework for the training programme (using a Logic Model approach) to identifying the intended outputs, impacts and outcomes of the training and to support a consistent approach to gathering data.
- Designing the evaluation framework. Design of the evaluation tools to gather data to evaluate the impact and outcomes of the training courses.
- Collection and analysis of quantitative data: To include anonymous output data, on participants (name, organisation, gender, age, ethnicity, geographic location), supplemented by pre and post surveys of participants, knowledge, understanding, confidence and future intent.
- Collection and analysis of qualitative data: Pre-training interviews with commissioners and training providers to explore needs and aspirations of the training; Post training interviews with the training leads to understand their thoughts on how the training was delivered and received; Post training participant focus groups with each of the three training programmes; Post-training interviews with identified stakeholders to assess perceptions of impact.
- Ethnographic data collection: Attending the three training programmes to observe and evidence the delivery of the training and the engagement of participants in the training.
Confidentiality: All participant data was gathered with participant consent and anonymised to ensure no personal identifiable data was gathered or stored. Where a participant did not consent to the sharing of data they were still able to partake in the training without prejudice. All data gathered as part of this evaluation is stored on secure systems is securely destroyed on completion of the report
3.1 The Outcomes Framework
The evaluators worked with Thrive LDN and training leads to co-design an outcomes framework for the programme (Fig 1). This was then utilsed to agree the evaluation measures – both qualitative and quantitative.
Fig 1: The Mental Health Recovery Mission Training: Outcomes Framework
4. The Programme Reach
This section of the report summarises the participant registration and attendance data. The data was taken directly by Thrive LDN from the Eventbrite registration system (with participant consent). The raw data was anonymised, before sharing with the evaluators for secondary analysis (no participant identifiable data was transferred).
4.1 Participants registered
In total, 2,373 unique participants registered on the three training programmes, with almost two thirds (63%) registering for the Trauma Informed Practice training. Twenty percent registered on Mental Health Awareness and 17% on Core Conversations training.
As the Trauma Informed training was delivered as pre-recorded session, there were no limits to the numbers that could register whereas the other two live programmes had a limit on the numbers able to register and this will have affected the total numbers registering per course.
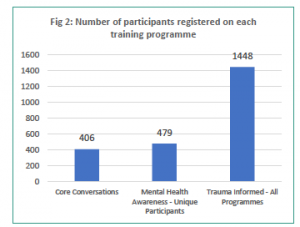
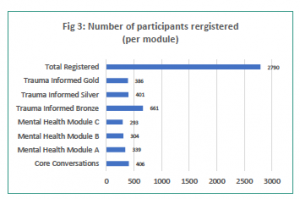
Two of the programmes were delivered in modular format – allowing participants to attend more than one session. In total there were 2,790 participants that registered for each module/course (1,448 Trauma Informed, 936 Mental Health Awareness and 406 Core Conversations).
Each of the two modular courses saw participants decrease from the first to the third sessions, with Trauma Informed participant numbers decreasing from 661 for the Bronze level to 386 for the Gold (53% decrease), whilst the Mental Health Awareness participants had a much less significant drop of, falling from 339 for Module A down to 293 for Module C (15% decrease).
The data indicates that the biggest fall off in registrations for both courses was between the 1st and 2nd modules (49% Trauma Informed and 11% Mental Health).
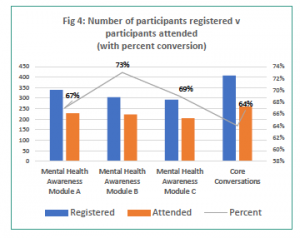
Not all registrations actually attended the training (converted from registration to attendance). Of the 1,342 participants registering for the three Mental Health modules and the core conversation training, 914 participants actually attended. Similarly with the Trauma Informed training, of the 1,488 participants that registered there were 1,254 unique viewers a conversion rate of 84%.
Across the three programmes combined, there was an average conversion rate from training to participation of 68%. This is a high conversion rate for webinars, with research indicating an average conversion rate for a free training programme would be just 55% (20).
4.2 Participant demographics
Training participants were predominantly female (83%) with just 13% stating their gender as Male. 4% preferred not to specify their gender.
Whilst this may suggest that males are less likely to register for training in this area, to some extent it perhaps reflects the workforce with two thirds of third sector workers nationally being female (21) and over 80% of the social care workforce are females (22).
Almost half (45%) of participants worked in the third sector and 35% in the public sector. Only 6% of participants worked in the private sector, with the remainder tending to work for education providers.
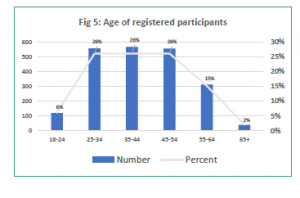
The age range of participants reflected the working age population, with 78% of participants aged between 25 and 54 years. Just 38 participants (2%) were aged over 65 years and just 118 participants (6%) were aged 18-24 years.
Again, this data is reflective of national level data on the age profiles of public and third sector workforce (23).
4.3 Participants role in supporting people with poor mental health
The training was accessed by people in a position to support others, building capacity to increase support for people with mental health problems.
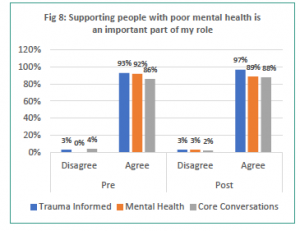
93% of Trauma Informed, 92% of Mental Health Awareness and 86% of Core Conversations participants agreed that supporting people with poor mental health was an important part of their role. These figures increased further post training for Trauma Informed and Core Conversations whilst for Mental Health Awareness it fell slightly.
“Trauma informed care is everyone’s business and, in order to make services trauma informed, these training sessions are very important” (Trauma Informed participant)
Participants who suggested that supporting people with poor mental health was not a key part of their role reported that it is still a key part of enabling them to offer support to others, outside of work.
“I do not support people with mental health issues in my role… I did the training for personal reasons as my son had a mental brake-down… I am glad I did the training. The fact mental health is now being spoken about a lot more is a positive move in the right direction. I feel it is still a hard subject to approach when someone is not ready to deal with it and for me this is where I wanted more guidance and information.” (Mental Health Awareness participant)
20 https://communications.on24.com/rs/848-AHN-047/images/ON24_benchmarks_20200309.pdf
21 https://cfg.org.uk/knowledge-hub/championing_gender_equality_in_the_third_sector#:~:text=Women%20make%20up%20two%2Dthirds,workforce%20within%20the%20third%20sector
22 https://www.theguardian.com/local-government-network/statsblog/2012/aug/07/employment-trends-women-local-government
23 https://www.ncvo.org.uk/news-and-insights/news-index/uk-civil-society-almanac-2021/workforce/who-works-in-the-voluntary-sector/#/
5. The Programme Impact on Participants
Through pre (immediately prior to the training) and post (immediately on completion of the training) surveys, we looked to understand the impact of the training on participants knowledge, confidence and attitudes.
5.1 Changes in participants knowledge
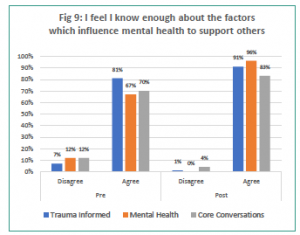
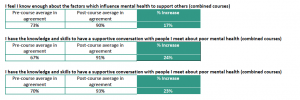
Prior to commencing the training, the majority of participants felt that they had enough knowledge about the factors that influence mental health. Eight in ten participants of the Trauma Informed training and seven in ten participants for the other two programmes agreeing to this.
The training clearly impacted on the majority of participants who did not feel they had sufficient knowledge at the outset. Post-training, 91% (Trauma Informed), 96% (Mental Health Awareness) and 83% (Core Conversations) participants reported they had enough knowledge. This is an increase in knowledge of between 10% and 29% of participants and clearly demonstrates that each training programme was effective in increasing participant knowledge of the risk factors which influence mental health.
Table 2: I feel I know enough about the factors which influence mental health to support others (combined courses)

“I learnt so much. It introduced me to a whole range of techniques and strategies which will help me in the future to recognise poor mental help and be able to provide information, support and guidance to the participants” (Mental Health Awareness Participant)
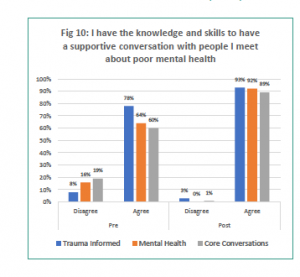
Whilst still high, fewer participants felt they had the knowledge to engage people in supportive conversations pre-training. Sixty percent (Core Conversations), 64% (Mental Health Awareness) and 78% (Trauma Informed) participants agreed that they had this knowledge before embarking on the training.
There was a significant increase in participants knowledge and skills in having a supportive conversation post training. There was an average of 91% of participants (across the three programmes) agreeing that they had the knowledge and skills post training. This was an increase in knowledge of between 15% and 29% of participants.
Table 3: I have the knowledge and skills to have a supportive conversation with people I meet about poor mental health (combined courses)

Perhaps reflective on the high levels of knowledge of participants at the outset and how the training was marketed some participants suggested that the training was too basic for them.
“I was disappointed at the level of this training, as for me it was too basic. However, it is a good starting point for those who do not have any formal training or experience in this area.” (Core Conversations participant)
“Perhaps this should have been promoted as an introductory level for those new to this type of work. I was expecting something more advanced.” (Core Conversations participant)
5.2 Changes in participants confidence
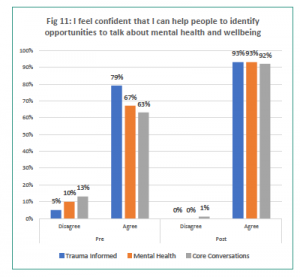
Around two thirds of participants felt confident in identifying opportunities to engage in conversations before attending the training – ranging from a low of 63% (Core Conversations participants) to a high of 79% (Trauma Informed participants). On average just one in ten participants (across the courses) did not feel confident in identifying opportunities. The remainder were neutral.
Across all three programmes there was a significant increase in the confidence of participants immediately following the training. Confidence in identifying opportunities increased to between 92% and 93% of participants feeling confident in identifying opportunities.
“The training and group-work conversations really helped to practice the learning. It left me feeling more confident to at least open discussions about mental health and identify how to help someone that may be struggling with their mental health” (Mental Health Awareness participant)
Table 4: I have the knowledge and skills to have a supportive conversation with people I meet about poor mental health (combined courses)

The pre-post survey explored how confident participants would be in supporting the people they had identified as suffering from poor mental health.
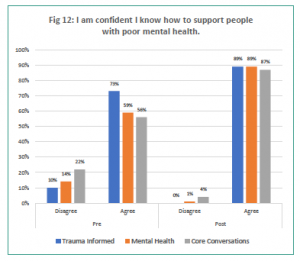
At the outset between 56% (Core Conversations) and 73% (Trauma Informed) of participants agreed that they had the confidence to support people, with between 10% and 22% not having the confidence. Post-training there was an increase of between 16% and 31% of participants feeling confident. Post training, approximately nine in ten participants felt confident to provide support to someone they had identified.
“The course was informative and I am more confident in working with the people who are trauma affected.” (Trauma Informed participant)
Table 5: I am confident I know how to support people with poor mental health (combined courses)

5.3 Changes in participants awareness of supporting resources
A key aspect of supporting people at risk of mental health problems is knowing how to advise and signpost people to appropriate support or resources.
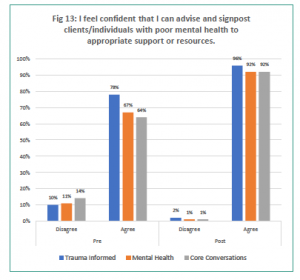
At the outset 64% (Core Conversations) 67% (Mental Health Awareness) and 78% (Trauma Informed) were confident in advising and signposting clients to appropriate support.
Post training these figures had risen to between 92% and 96% of participants feeling confident to advise and signpost individuals with poor mental health to appropriate support or resources.
“The training made me understand that, although I am not specifically trained, I now have awareness of trauma and knowledge of tools to support people” (Mental Health Awareness participant)
“This improved my awareness and my sensitivity towards mental health issues and well-being in general.” (Trauma Informed participant)
Table 6: I feel confident that I can advise and signpost clients/individuals with poor mental health to appropriate support or resources. (combined courses)

5.4 Changes in participants practice
The real impact of any training programme is if the participants take their increased knowledge and confidence and translate that into changing their practice. However, the post training surveys were completed immediately following the training – not allowing sufficient time to quantify impact. Therefore, the evaluation took an interim measure of intent, comparing participants levels of engagement in supporting people with mental health issues at the outset and their reported intent to support individuals post training.
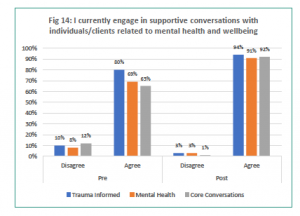
Between 65% (Core Conversations) and 80% (Trauma Informed) engaged in supportive conversations with clients before embarking on the training. Post-training between 91-94% of participants stated that they have supportive conversations with individuals/clients related to mental health and wellbeing, an increase of 21% of participants across the three courses.
Table 7: I currently engage in supportive conversations with individuals/clients related to mental health and wellbeing (combined courses)

5.5 Participant views on the effectiveness of training delivery
“The training introduced me to a whole range of techniques and strategies which will help me to recognise poor mental health and be able to provide information, support and guidance to the participants.”
(Mental Health Awareness participant)
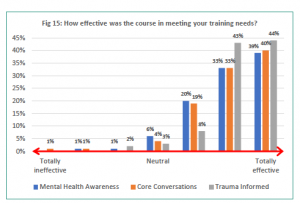
The reported effectiveness of all three training programmes in meeting the learners needs is very high. Over seven-in-ten participants of the Mental Health Awareness and Core Conversations training and nine-in-ten of the Trauma Informed participants rating it ‘very’ or ‘totally’ effective.
“I am a Councilor and Mental Health First Aider and I run my own community support group for female survivors of domestic abuse. I felt the training was very impactful in helping me to develop my softer skills and considering how my approach is making the client feels which can then impact on the client’s level of engagement.” (Core Conversations Participant)
“I have done a fair few training programmes, but this one seems to explain things in a way that makes more sense to me… things about PTSD the stories of people and human connection struggles. It’s less medical sounding than many others. (Trauma Informed Participant)
Just 2% of Core Conversations and 1% Mental Health Awareness participants found the course ‘totally’ or ‘very’ ineffective. The reasons behind these ‘ineffective’ ratings related to the lack of depth provided within the training.
“I didn’t feel the course was suited to what I wanted to get out of it. I was looking more detailed advice on how to look/deal with mental health in the work place.” (Mental Health Awareness Participant)
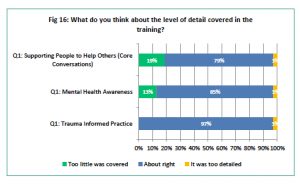
Most participants reported that the level of detail covered within each of the three training programmes was about right in meeting their training needs.
However, 19% of Core Conversations and 13% of Mental Health Awareness training participants reported that there was an insufficient level of detail covered on the course. This potentially could link back to the high levels of participants existing knowledge before enrolling on the training.
“I found the training very basic. Due to my social work background, it was not helpful in extending my knowledge in this area.” (Core Conversations Participants)
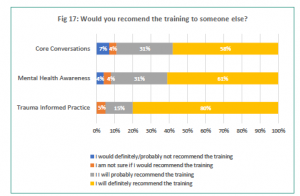
A true guide to participants views on the training is if they would recommend it to someone else.
Clearly the Trauma Informed Practice training was very highly regarded with 80% of participants saying that they would ‘definitely’ recommend it and zero responders saying that they would ‘not’ recommend it.
Whilst responses to the other two training programmes was very positive, they had fewer participants ‘definitely’ recommending the training to others (58% – Core Conversations and 61% – Mental Health Awareness) with 31% of both saying they would ‘probably’ recommend it.
“I thoroughly enjoyed the course and found Nicola Lester’s approach very engaging. It has encouraged me to better value the work my team does within the hospital, which often goes unrecognised… and collaboratively problem-solve the systems and practices that are (unintentionally) harming staff.”
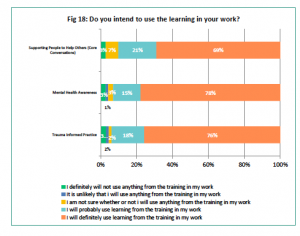
Following the training, participants were asked if they intended to use the learning in their practice.
Responses across all three programmes indicated a strong willingness to use the training in their practice with 78% (Mental Health Awareness), 76% (Trauma Informed) and 69% (Core Conversations) participants saying that they will definitely use the training in their work. A further 15-21% of participants stated that they will probably use the learning in their work.
Just 3% of participants from each of the training programmes stated that they will definitely not use the training in their work.
6. Training Programme Focus Groups
To help understand the impacts that the training programmes had on participants (post-training) we delivered three focus groups of participants at 3-6 months post completion of the training. The focus groups were delivered as facilitated on-line sessions, with 42 training course participants. The data presented in the case studies below is reflective of the views of each group.
6.1 Case Study 1: Mental Health Awareness Training
Promotion of the training offer
There were mixed views on how the training programme was promoted. To some participants it was promoted in combination with the other two training offers whilst others were unaware of the additional training. Participants suggested that it would have been helpful if each participant had been made aware that there was complimentary training and suggested that all courses should have been branded together.
Delivery style and content
In general participants reflected that this training exceeded their expectations.
‘”I’ve done a lot of mental health training and over the past 3-4 years, since COVID started… I think this was one of the better ones that I’ve ever experienced.”
“I thought it was a good complement to what I did in the past and it was helpful in a way to self-reflect on yourself how we do things… how we are sometimes being a bit too just judgmental……. that was one of my problems and so I’ve learned to be less judgmental …”
Participants valued the targeting of the training programme specifically to London boroughs, rather than it being delivered across a wider geography. They suggested that this created a space for shared understanding of the issues facing local people, generated opportunity for peer-peer learning and helped to develop their local professional networks. They reported that in most cases the interaction between participants has continued post training.
“It was really valuable that this was specifically about London….. the fact that training was geographically specific was the real draw for me… I’ve made some great professional contacts”
There were mixed views on the interactive (group work) delivery style. Most of the participants valued the breakout sessions, reflecting that it supported participant interaction. However, the training style did not suit all participants with some reporting the group work was too intense and stating that they would prefer pre-recorded videos demonstrating the techniques rather than role-play breakouts.
“It was great to just hear the lived experience of so many different practitioners across lots of different sectors, which I think, as people on the frontline dealing with individuals, can help us feel less isolated and help us as practitioners. We’re not alone in trying to tackle these issues.’
“I think it was very interesting to be a with other participants who were facing different issues because of a different involvement with their communities. That helps me to reflect on how they were dealing with a certain situation… I think the breakout rooms were very good for that.”
Participants suggest that it would have been helpful to have videos and other training materials circulated in advance of the training to allow them to better prepare for the course.
Impact of the training
Participants were very positive about the changes that the training had made in practice 3-6 months post training. They highlighted the ‘real-life’ impact of the training on their ability to engage people in difficult conversations. For some it had been about reassurance that their approach was correct, whilst for others it had made them realise appropriate methods of how they should identify and engage people who need support.
“I have people crying in front of me. Before the training it used to be a bit awkward, like oh, you know what do I do…Now it’s more ‘right quick tissue, don’t worry, we can help you back.’ There are ways to talk to them, ways of giving them advice and tools for them to take away. So I really do think that it has helped me to understand that there’s a lot of people out there dealing with their own mental health.”
“I needed to be more confident in in dealing with difficult issues, and that’s why I registered with a few new programmes recently. As a result of this training, I’m going to start as a food bank Assessor, which I wouldn’t have done before, if I hadn’t done the course.”
Future training
Generally all participants highlighting the need for additional training/professional development in this field. Whilst not specific on the types of training they required (several topics were suggested), they all requested a refresher programme to ‘cement the learning’.
“I would like to see more of training that is available. I also feel like refresher trainings should be available.. With regular training every six months or four months.”
6.2 Case Study 2: Core Conversations Training
Promotion of the training offer
Participants felt that the promotion of the training did not sufficiently explain the style of training delivery. In particular, participants felt that the role play elements of the training needed emphasising on the promotional literature.
It was suggested that simple changes to the promotional materials could help engage a wider workforce. They felt that the programme is suitable for a wide range of roles but was predominately attended by those already working in the field. It was suggested that the promotional literature needs developing to highlight the breadth of roles that could benefit from the training.
“Some of the language used to describe the workshop might not engage with some types of staff eg IT/HR. Use of ‘role play’ and ‘acting’ might put people off.”
“I can see how this would be useful for staff in a range of different roles around our Council, so that’s how we’re kind of embedding it, hopefully within the work of the Council. Because the training is quite generic, it can be used in lots of different departments as well, which is really useful.”
Delivery style and content
Participants reflected very positively on the training programme. Most were particularly appreciative of the delivery style, in particular the interactive and reflective nature of the training. However, some suggest that role-play is unique to a particular learning style and can be very off-putting for others. It was suggested that the training would benefit from an additional, shorter introductory session prior to this training – to allow participants to familiarise themselves with each other and the delivery style.
“Role play with a group of strangers can be uncomfortable.. [there was] a huge expectation for a group of strangers to come in so quickly and do that kind of activity and particularly online as well.”
“I thought the training style was unique and a different way to learn. With different techniques to have those core conversations with individuals who are in a vulnerable position.”
Participants reflected favorably on the ‘unique’ and ‘effective’ training style. They valued the opportunity to share ideas with peers and to learn from the experiences of others within the group.
“What I loved was that we, as participants, were the ones making.. the assessment, the judgments about what was done and whether or not we would shift or change something.”
“….sharing ideas back and forth… how we are going about stuff, if we had questions. We had a little group where we could bounce ideas and ask what other people thought.”
Some participants felt the content had to be rushed through, due to time limitations of a one -off session and that there was a need for perhaps extending the training.
“The first session in particular did feel quite rushed. The way we did it, introductions and then like you’re in a breakout room, then you go in another breakout room.”
All participants were complementary about the facilitators.
Impact of the training
Whilst the majority of the group reflected that they already felt confident to have difficult conversations prior to the training they suggested that it had offered them additional tools to utilize within their professional interactions. The group suggested that the biggest impacts had been around developing active listening skills and enhancing their confidence to hold conversations in different types of settings and in difficult situations.
“There’s the growth in my confidence, but what appealed most was just a new, unique and different way… to engage individuals in a what could potentially be a difficult conversation.”
“The training supported the nuances of how do you elicit information from somebody… [whilst]maintaining their privacy and confidentiality…”
In the months since training, participants had either started to have more difficult conversations with clients or had ‘tweaked’ the way they have these conversations, making them more personable or more effective.
“Sometimes the person in front of you is behaving in a way that you don’t perhaps identify and it’s very unusual. …. the core conversation [training] was excellent in ensuring [I’m]not making assumptions.”
“The training has helped me to step back and to not rush into things. You can’t solve everything, especially not in the first conversation, but being there for somebody… showing that you have empathy.”
Additional training
There is a desire to build on the training and increase the offer further, in particular more training and resource on where to signpost people to and a consistent request for more follow up sessions to be made available.
“It would be useful to have specific details of where individuals can be signposted to, both by referral and also self-referral if necessary.”
6.3 Case Study 3: Trauma Informed Practice Training
Promotion of the training
This training programme differed significantly from the other two, as it was delivered as a pre-recorded session. The links for the training were initially promoted at prescribed dates and times for the participants, but they were also available for viewing outside of these times and still remains live. 23
Participants reported that they had initially thought they were attending a live session. They suggested the pre-recorded nature of the training should have been clearer within the marketing. Some participants suggested that if they had known it was a pre-recorded session they would not have initially joined, however, they went on to say how pleased they were that they had actually taken part.
‘I was expecting it to be live. That there was going to be a physical trainer and we were going to reflect together and think about experiences… So, when it was a video, I was a bit surprised”
‘I probably wouldn’t have [joined] if I had known it was pre-recorded… If I’d known it was like a YouTube video I wouldn’t have joined if I’m really honest.’
Delivery style and content
Participants found the delivery style of pre-recorded sessions both helpful and engaging. It provided participants with the opportunity to pause the training, to revisit it at later dates and to fit it around other work commitments, allowing for greater reflection on the learning.
“I was surprised [that it was pre-recorded] but then I was thinking … oh, I can pause this and play it back later, so I don’t need to be here at this time.”
“The training delivery style allowed me to be very reflective and introspective … about how I was to use it within my practice as well.”
Whilst none of the focus group participants had needed to utilise the sign-language feature available with the training, they thought this was a really helpful addition and made the training feel ‘more live’.
Participants found the content extremely engaging and stated that they found the presenter easy to listen to. They particularly drew reference to the links to other supporting resources and references for participants to follow up on.
“I did find it helpful and very informative and all the diverse references to different books and videos was helpful.”
The option to progress through three connected yet separate modules (Bronze, Silver, Gold) was greatly appreciated by participants, as it gradually built on their knowledge from the previous session in bite sized chunks. Participants really enjoyed this delivery style and would certainly attend other pre-recorded sessions and recommend this course to colleagues.
Impact on participants
Participants highlighted the positive impact the course had on their subject knowledge and their confidence in putting the training into practice. They appreciated the ‘professional accreditation’ it gave them. In particular, participants highlighted the personal impact of the training and the influence it has had on their interactions with people they come into contact with both inside and outside of work.
“The course came a time I was made redundant. So it’s kind of put a few things into perspective for me personally as well.”
“If somebody’s shouting and screaming and swearing in your face … sometimes there’s ‘hostility…, and then [you] to form a view about a young person… a sticky label. The training helped me to think about it from another perspective.”
“I work in an NHS hospital supporting staff 1:1 and in groups for training and reflective practice… The skills and knowledge highlighted on the course are woven throughout my work and inform every interaction. Whilst some of the concepts were not new, the course has extended my understanding, practice and confidence.”
“[I’ve learnt some] transferable skills that I can use in different settings whenever I’m working with young people or with adults… I think what it has done is to empower me when I’m working with certain communities. I’ve got a framework I can work towards where they can see a trust process. I’m not telling them it will work for them or it won’t work for them, but there’s that process that it is clear you can work through that it’s easy to pass on to your client.’
Further training
The group felt that it would be useful if the training course was available in other languages – reflective of the London boroughs and felt this would be a natural progression for the future and one which a pre-recorded session could lend itself to.
Participants suggest that there was potential to expand the training offer to highlight trauma in specific London population groups including temporary students and refugees who have a broader definition of trauma.
“I work with refugees, migrants as well. Amongst our residents are those people that have come from war torn countries that have PTSD that are really suffering. This is a broader definition that could be considered.”
“I feel they [older men] carry the most stigma in terms of awareness / acknowledgement of their mental ill health. It would be good to have support/training in regards to that particular demographic.”
7. Discussion
Co-design of training package
Thrive LDN worked hard at the outset to ensure that there were clear synergies between the training programmes. They came together with the three training providers at the outset of awarding the contracts to discuss the content and it was agreed that they would have a trauma informed thread running through them and framing the promotion around the concept of having difficult conversations.
Through ethnographic visits by the evaluators to each of the training packages we were able to evidence that there was clear synergy between programmes, making them feel like a coherent package of training.
“I think it was targeted to the people who were in those sort of community roles, whether informal or formal roles and there’s quite a bit of work that went into promoting through our networks … I think the key bit for me anyway is actually working with the providers.” (Commissioner)
This approach is to be applauded and the willingness for separate training providers (who may compete for tenders in this area) to work together to co-produce materials.
Part of the ask for the service providers was to see how the training could be sustainable. It is very encouraging that sustainability of the training offer was considered from the outset. For two of the programmes there is an online link that people can continue to access the training going forward. For the third one, a train the trainer programme was delivered with local authorities. It would be worthwhile revisiting this in the near future to understand if these opportunities are still being taken up.
“And so I think for us, we have done quite a lot of research, and we’ve delivered quite a lot of training packages in the past that were not sustainable post funding. So we were quite keen on this occasion to have something sustainable longer term” (Commissioner)
“The key learning for us was to have something that we could continue to support Londoners with going forward and actually with this, we can continue to signpost to that training.” (Stakeholder)
Marketing and promotion
Thrive LDN took a cascade approach to promoting the training and they recognised the limitations of this approach. The approach was limited by a lack of budget for paid marketing and so they were primarily reliant on word of mouth in promoting the training. This included working with key regional networks and local authority partners.
Rather than promoting all three programmes collectively they took a staggered approach across a number of weeks. Whilst the approach was evidenced as effective by the high take up the programmes, participants fed back that they would like to have been aware of the other training offers and were disappointed that they had missed some of the communications around this.
“The approach meant that we could take a targeted approach other for example the Turkey Syria earthquakes in February. The trauma informed practice was up and running and so that was actually shared as a resource for those working in the communities that are most affected in London, as a resource that they might want to participate in to help with the role.” (Stakeholder)
Geographic targeting
It is of note that some training programmes were targeted at specific London boroughs, whilst other were delivered pan-London. This may reflect the variance in numbers attending training from the various boroughs. There was low take-up by participants from certain boroughs with higher rates of mental health problems for example only 31 participants worked in Tower Hamlets, 17 from Waltham Forest and 43 from Barking and Dagenham and these boughs have the 3rd, 5th and 6th highest prevalence rates of Common Mental Health Disorders respectively. This perhaps requires further consideration of future training offers to ensure greater targeting in boroughs with higher mental health prevalence.
It was also reported that drop out (from registration to attendance) was higher on the pan-borough programmes, which indicates there was a greater buy-in for borough specific programmes.
“I think we initially thought the pan London would be a catch all for those that haven’t been able to do the sessions, which they were, but I think there was a higher drop off rate for the pan-London ones than they were for the borough specific ones. So maybe it would have been more beneficial to maybe target those boroughs with low uptake” (Training Provider)
Programme demand
There was a very clear demand for the training programmes – evidenced by the number of participants signing up and the range of organisations represented. Signups for each course were completed quickly and stakeholders talked about the importance and effectiveness of working with local authorities and having a local authority lead to identify organisations that would then take the training. Many courses had a waiting list which suggests that there is still unmet need across London.
“It definitely exceeded what we wanted. I mean, just for example with Core Conversations training, when we released the last two pan London sessions, they almost snapped up within 24 hours for the attendance. So there was definitely a need out there.” (Commissioner)
Knowledge of participants prior to training
The evaluation found that the majority of participants already had extensive experience and knowledge in the subject matter which suggests that it may not have been effective in engaging participants new to the subject. Discussions with stakeholders suggest that at the outset they would have expected more people to attend the training with limited knowledge of the subject matter – allowing them to be upskilled. There was discussion relating to whether the content of the training programmes could have been clearer at the outset so fewer participants, who already had that knowledge, would have participated in the earlier modules and joined the training at intermediate and advanced levels. Going forward there is an opportunity to define the level of training more clearly and reach out to people new to the workforce.
“And there was always the sort of understanding that there would be quite a wide a broad group of people attending any one session so there may be someone that hadn’t done any training before and someone that had done some.” (Commissioner)
“So maybe we could have been slightly more detailed into their what was in there, although I think in the columns that went out it was quite clear what was actually within the modules.” (Commissioner)
However people attending the training with a high knowledge of the subject, meant that there was a significant opportunity for participants to share their knowledge and experiences and generated significant peer-peer learning.
Impacts of the training provision
The evaluation has evidenced significant short term impacts of the training on participants knowledge and confidence and their intent to put the training into practice. Despite participants arriving on the training already having high levels of knowledge and confidence, there was a positive increase in levels across all domains evaluated.
There was also a clear demonstration of participants using the training to cascade to a wider audience within their local area or within their own organisation. The evaluation did not gather evidence to quantify this reach (it was outside of the brief) but qualitatively participants talked with enthusiasm about how they have shared the learning.
“I went to a session after the [Core Conversation] training had been completed with the training provider, and the individuals from the local authority that had been identified as the trainers. It was just incredible to see how many of those individuals had actually delivered training sessions… for some of the individuals that hadn’t delivered training before, I guess the impact on themselves to learn these new skills, and then also the impact that then has on the community because actually we’ve upskilled these individuals and then they’re continuing to deliver the training so that was really great to see for me.” (Stakeholder)
“As a chaplain, I was already conscious of the idea that an organisation has a collective soul, and found this part of the gold level course fascinating. The course has helped provide me with a psychologically-based language to raise the idea of embedded trauma with colleagues within the secular / scientific context of the hospital. This is important at a time when the NHS and the staff who work for it are under huge pressure and at risk of moral distress and injury.” (Participant)
In terms of the wider impact of participants utilising the training in practice, the timescales for this evaluation made this problematic to quantify. We therefore agreed on the short term measure of considering participants intent to utilise the training to support others. Over 90% of participants across each of the training programme gave a strong indication that they intended to use this training to support others.
The post training focus groups indicated that the reported intent was being turned into practice. The majority of participants across all focus groups gave clear concrete examples of when and how they had utilised this training.
“I work with a volunteer group one of whom sadly passed away earlier this year. I have used some techniques from the training to talk to the volunteers sensitively about it.” (Participant)
“I’d say that I was using the approach and mostly using the principles presented in the training into practice as much as possible within my role already. That said, there’s a limit to the extent I can do so, due to the physical set-up of my project.” (Participant)
“For me, the key impact is around maintaining awareness of the sensitivity of some conversations, and trying to facilitate the most privacy and dignity for the person possible when having such conversations. In that respect, it means that the person feels more ‘cared for’ / attended to, and I feel better for that reason. I also feel more confident to acknowledge / be clear about the extent of my remit, so not ‘over-promising’, and able to contain the individual’s expectations.” (Participant)
“I now view my work through a trauma informed ‘lens’ so am more sensitive and less likely to jump to conclusions about an individual’s responses to challenge.” (Participant)
Longer term follow up of participants however is notoriously difficult and response rates to long term follow up surveys would be anticipated to be very low. This is not to say that it should not be attempted and perhaps, through incentivising participation, more quantifiable longer term data could be generated.
It is finally worth reflecting on the independent evaluation process. All too often evaluators are brought in towards the end of the programme and this severely limits the evaluation. However, Thrive LDN brought the evaluators in at the outset of this programme. This enabled the evaluators to work with stakeholders to agree an outcomes framework for the training and set a pragmatic approach to evaluating the outcomes that work for providers and participants.
“I think it’s very useful for you [Evaluators} coming in at an early stage and speaking to the providers, knowing that we’re having that external evaluation, and sort of working together as a unit more so than just all individual, I think was really helpful.” (Commissioner)
Having the evaluators embedded meant that the emerging findings could be reported through to the providers in real time. This enabled the training to be tweaked to meet participant needs and allowed the approach to evaluation to be adapted mid-programme, changing the method and delivery of the pre-post surveys and incentivising post survey responses.
“I know the first few sessions we didn’t do it, but getting the providers to post the pre surveys at the beginning of the sessions and the post surveys after the sessions really helped me to get some more feedback from people within the sessions because they were doing it there and then.” (Commissioner)
“The live feedback we got from the pre-post participant surveys led us to adapt the training after the first few sessions. Not major changes in content but tweaks to the delivery style. This really improved the programme from a participant perspective” (Training Provider)
8. Conclusions and Recommendations
This report has demonstrated that the Thrive LDN Mental Health Recovery Mission training programme funded by the Mayor of London, achieved the original aims and objectives of the commissioned programmes. The training provision successfully engaged a wide range of participants from across all London Boroughs in supporting people with who they come in to contact.
The varied training offer and delivery style that each programme took ensured that a range of learning styles were catered for, which increases the likelihood of the programme leaving a legacy within participants delivery organisations.
A majority of participants across all three training programmes reported increased knowledge and confidence and have therefore been ‘empowered’ to support people who they come in to contact with who are potentially suffering from mental health issues. The evaluation has found clear evidence of participants putting the learning into practice and therefore anticipates that it will be having a positive impact on the lives of many Londoners suffering from mental health related problems.
Nevertheless, some key challenges to various elements of the programme have been identified in this report, including:
- some aspects of the way in which the programme has been promoted/marketed
- it’s limited reach into certain boroughs that have high levels of mental health amongst their populations
- and in quantifying the way in which the training has positively impacted the participants practice post training.
Some fine tuning to the training offers, going forward, could therefore ensure that its reach and positive impact in practice is even more widespread in the future.
8.1 Recommendations
This final section now considers some of the implications of these findings on the programme as a whole, providing six broad recommendations.
Recommendation 1: Continue to provide a training offer in this field
There is a growing body of evidence that health inequalities are now widening and that the cost-of-living crisis, poverty and financial stress will likely rise over the next few years. The Mental Health Foundation report that the effects of the cost-of-living crisis on public mental health will be on a scale similar to the COVID-19 pandemic and that concerns about finances are having a negative effect on people’s ability to engage in some of the activities known to help protect mental health.
Further, the high uptake for the programme has clearly demonstrated an on-going need amongst practitioners who support vulnerable populations. We would therefore recommend that the training offer, or similar, should be continued, including a refresher training programme for participants already engaged. There should be consideration as to the sustainability of the training programme in the longer term.
Recommendation 2: Further develop the marketing and promotion of the training
In terms of promoting individual training programmes it is clear that the promotion reached an appropriate audience in general, although it was less successful in engaging those with limited knowledge and confidence and this should be considered in any future promotion to ensure it upskills a wider workforce.
There was significant differences in the numbers of participants attending from different boroughs and some boroughs with high levels of need were under represented. Perhaps one of the biggest challenges to the programme, in working across such a high number of boroughs, was on the reliance of word of mouth to cascade the training, which in itself is reliant on having key proactive contacts within each borough.
Moving forward it may be worth bringing the training courses under one marketing/promotional banner, rather than having three independent offers. For example, whilst feedback around the individual training was very positive, many participants did not appreciate that there was more than one training option that they could access. Linking training programmes together may also assist in securing future funding, identifying gaps in meeting need, or perhaps jointly running the programmes to reduce cost.
Recommendation 3: Minimising programme drop off
Whilst this report found a high rate of registrations attending the training (68%) there were still 428 participants who registered on the Core Conversations and Mental Health Awareness training that did not attend. For both of these training programmes numbers were limited to a maximum attendance rate – so this often meant that programmes were ran under capacity, in particular the pan London programmes.
Whilst keeping the training free for attendees, to minimise drop out between booking and attending organisations should consider the introduction of a charging policy, for participants who register and then do not turn up for the training. Whilst it is reported that this may be problematic under current systems within the NHS, it is nonetheless worth considering systems to maximise attendance of those registered.
Recommendation 4: Broadening the training offer
Participants consistently requested additional training opportunities linked to supporting people suffering from mental ill-health. They talked for example about specific population groups, e.g. those from certain ethnicities, males, students, veterans and others or on specific settings such as the workplace. There is also potential for delivery of the training in non-English languages and this could also be investigated further.
Whilst Thrive LDN continue to develop a broad training offer it may be helpful to reach out to participants from this training programme to gauge interest in developing more specific offers for the future.
Recommendation 5: Develop the evaluation methodology to gather longer term outcomes
Whilst this report has highlighted difficulties in long term evaluation of impact, the real impact of the training offer lies in the use of the training to support people within communities. It is certainly worth considering how this can be achieved over the coming months through reaching out to participants – either through a short survey or potentially developing participant case studies.
The way Thrive LDN built the evaluation in to the training at the outset is to be commended and is a model of good practice that Thrive LDN should continue to follow for other significant contracts of work. To some extent, this may be limited by budgets, however the principles followed within this evaluation could be applied internally.
Recommendation 6: Share the learning
This evaluation is of interest to a wide range of audiences, including others commissioning and delivering related training. As such we would recommend that the report is widely circulated and presented to key stakeholders locally and nationally.
9. Acknowledgments
- Thrive LDN gathered the core output data used to assess reach. They were responsible for helping to circulate the e-survey links and connecting the evaluators with key partners
- The training providers: Basis, Healthy Dialogues and Nicola Lester have supported the evaluation throughout, supporting the process and outcome measures through the distribution of e-survey links, pre and post interviews with evaluators and utilising the emerging findings into developing the training offer.
- ‘Mayor of London and Mental Health: The training programme was funded by the Mayor of London. The Mayor’s ambition is that Londoners share in a city with best mental health in the world. By speaking openly about his own experiences and encouraging others to do the same, the Mayor seeks to challenge mental health stigma and remind Londoners that they are never alone’